Dear SDOH Colleagues:
The Number Needed to Vaccinate (NNV) has not customarily been used in Public Health, because it is so dependent on the underlying chances of infection and of the outcomes of interest.
EXAMPLE: If the vaccine series is 90% protective against outcome X, which occurs in 2% of infected patients, and the chance of infection is 1% over the time period being analyzed, the NNV to prevent that outcome would be 1/(0.9x0.02x0.01) = 5,556.
Now I’ll change just one variable. If the vaccine series is 90% protective against outcome X, which occurs in 2% of infected patients, and the chance of infection is 90% over the time period being analyzed, the NNV would be 1/(0.9x0.02x0.9) = 62, just from the change in population infection rates.
Choose a different outcome, you get a dramatically different NNV. Choose a different time frame for outcomes, you might get a very different NNV.
Plus, comparing deaths among vaccinated people with deaths among unvaccinated people, the Number Needed to Harm (NNH), with respect to excess deaths after COVID vaccine, would be a very high number indeed, probably somewhere between 250,000 and several million.
***
An individual-level analysis such as NNV, when applied to a vaccine against an infection that is transmitted person-to-person, fails to incorporate whatever value the vaccine may have in preventing transmission to others. The “Number Needed to Vaccinate to Prevent One Transmission” would depend additionally on assumptions about the likelihood of transmission, about the exact effect of the vaccine on transmission, and on the downstream effect of vaccine in preventing subsequent cases.
For instance, 95-99% population coverage with measles vaccine will essentially eliminate all measles transmission in a society. Under those circumstances, the “NNV” would be extremely high for a time – but, if vaccine were then neglected because the NNV was high, measles would return and all children would be at risk again.
“NNV” would have serious meaning only for things like tetanus vaccine, because tetanus is caught from the environment and is almost never transmitted person to person (even in completely unvaccinated populations). For most other vaccines, you need a population analysis in which “NNV” has very little value.
***
Discussions of “herd immunity” from COVID-19 vaccines always depended on assumptions that the vaccine would prevent transmission by the same factor that it prevents severe illness and death. A reasonable assumption, given the behavior of other vaccines, but not accurate for COVID-19 vaccine.
Still, given the system load of COVID-19 patients, and given my own recent unpleasant experience with COVID-19, I’m grateful to every immunized person for minimizing the population burden of severe disease – AND I’m grateful to those who made three doses of vaccine available to me, which may have saved my life!
***
Thanks to discussants for a civil, and sometimes informative, discussion….
Best wishes!
Dave Cundiff MD MPH
Ilwaco, Washington, USA
*** *** ***
From: Social Determinants of Health <[log in to unmask]> on behalf of "Joanne G. De Montigny" <[log in to unmask]>
Reply-To: Social Determinants of Health <[log in to unmask]>
Date: Sunday, January 30, 2022 at 1:00 PM
To: <[log in to unmask]>
Subject: Re: [SDOH] Vaccines Work - NNV between 78 and 120 reference included, not 1000 that CS suggested
If I may, I would like to contribute a related response to your inquiry.
A recent news article, published on January 17, 2022, in The Times of Israel, announced preliminary results of a study on a fourth vaccine dose, being offered to Israelis in response to the Omicron wave. Prof. Gili Regev-Yochay, a lead researcher in this study, said that the vaccine for Omicron is “not good enough,” but should still be given to those at high risk, especially the elderly, “even though the vaccine doesn’t provide optimal protection against getting infected with the variant” [1]
The vaccine may still be protective against severe covid-19 symptoms, so it could be useful for those at risk of severe disease, mainly the elderly and immune-compromised. But, the virus has evolved to the point where the vaccine-generated antibodies (targeting the spike protein of the original viral strain) do not optimally recognize the spike protein of the new variant.
Covid-19 vaccines do not provide reliable protection against infection and transmission, but are now meant for therapeutic use. However, there are other options to keep infected people, vaccinated and unvaccinated, from clogging up hospitals.
On January 11, 2022, the World Health Organization’s Technical Advisory Group on COVID-19 Vaccine Composition issued a statement saying that “a vaccination strategy based on repeated booster doses of the original vaccine composition is unlikely to be appropriate or sustainable.” [2]
We cannot keep using the same strategy over and over again and expect different results. There are other solutions that need to be brought out into the open.
[1] The Times of Israel. (2022). Israeli trial, world’s first, finds 4th dose ‘not good enough’ against Omicron. Retrieved from
https://www.timesofisrael.com/israeli-trial-worlds-first-finds-4th-dose-not-good-enough-against-omicron/
[2] World Health Organization. (2022). Interim Statement on COVID-19 vaccines in the context of the circulation of the Omicron SARS-CoV-2 Variant from the WHO Technical Advisory Group on COVID-19 Vaccine Composition (TAG-CO-VAC). Retrieved from
https://www.who.int/news/item/11-01-2022-interim-statement-on-covid-19-vaccines-in-the-context-of-the-circulation-of-the-omicron-sars-cov-2-variant-from-the-who-technical-advisory-group-on-covid-19-vaccine-composition
Joanne de Montigny, PhD
From: Social Determinants of Health <[log in to unmask]> on behalf of David Zitner <[log in to unmask]>
Sent: Saturday, January 29, 2022 11:26 PM
To: [log in to unmask] <[log in to unmask]>
Subject: Re: [SDOH] Vaccines Work - NNV between 78 and 120 reference included, not 1000 that CS suggested
Attention : courriel externe | external email
Claudia, I am interested in hearing about the research that prompted your high estimate of NNV. Perhaps this is one reason for the confusion. Link below to peer reviewed article in Lancet Microbe.
The data suggests the vaccine is very effective, with very little harm. Perhaps your reference will suggest why some believe the vaccine is less effective.
COVID-19 vaccine efficacy and effectiveness—the elephant (not) in the room (nih.gov)
COVID-19 vaccine efficacy and effectiveness—the elephant (not) in the room
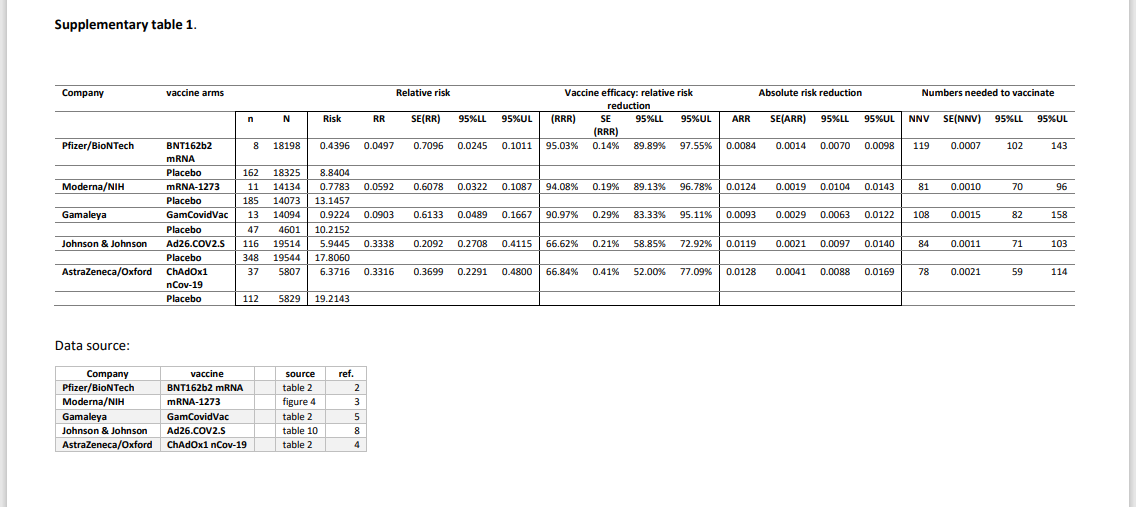
Approximately 96 COVID-19 vaccines are at various stages of clinical development.1 At present, we have the interim results of four studies published in scientific journals (on the Pfizer–BioNTech BNT162b2 mRNA vaccine,2 the Moderna–US National Institutes of Health [NIH] mRNA-1273 vaccine,3 the AstraZeneca–Oxford ChAdOx1 nCov-19 vaccine,4 and the Gamaleya GamCovidVac [Sputnik V] vaccine)5 ...
www.ncbi.nlm.nih.gov
From: Social Determinants of Health <[log in to unmask]> on behalf of Claudia Chaufan <[log in to unmask]>
Sent: Saturday, January 29, 2022 4:53 PM
To: [log in to unmask] <[log in to unmask]>
Subject: Re: [SDOH] Vaccines don't work
CAUTION: The Sender of this email is not from within Dalhousie.
To the point of the Guardian, it is people, not rates, that occupy beds at hospitals. Even if only one person in the UK or in Canada remained unvaccinated and ended up hospitalized or dead (100% rate of hospitalization/death for the unvaxxinated), could you really say that that one person is ‘clogging the hospitals”?
Health services experts know well that about 20% of the population consumes about 80% of health services. This is a feature of populations – in any population there will always be people who are older, have ‘bad’ behaviours so end up sicker (or are seen as having them depending on the politics of the times), or are sicker for whatever reason, and so on.
But I would think that most people in this forum do not go around moralizing about health behaviours, whether it is failing to eat healthfully, exercising, and losing weight, or to stop smoking, drinking, etc., however good these behaviours may be to increase several times your chances of not dying – to classify your patients between deserving and undeserving and refuse them care. In bioethics this issue has been settled a long time ago with the case of smokers.
More to the point, the ‘unvaxxed’ clogging hospitals? Not in Canada or the UK. The attached pictures from Public Health Ontario clearly show that most ICU beds are not-covid (57% vs. 21%) and that 27% of ICU beds are empty. And since Omicron, both case counts and rates have gone through the roof, apparently much more so among the double (or triple) vaxxed. There are a few interesting hypotheses out there that allude to how our complex immune system works.
In the UK (p. 43, 44 and 45 in the latest report), most cases, hospitalizations and deaths are ocuring among vaccinated patients (some even triple vaxxed). https://www.gov.uk/government/publications/covid-19-vaccine-weekly-surveillance-reports
Finally, if both vaxxed and unvaxxed have roughly equal viral loads and can transmit the virus equally (Secondary Attack Rates among vaccinated 25%, unvaxxinated 23%, so lower capacity to trasmit, the Lancet Infectious Diseases), in other way, you cannot separate ‘us’ from ‘them’ with vaccination, what is the public health rationale for mandates?
Let me set aside for now the issue of NNT and NNV (Numbers Needed to Treat and Numbers Needed to Vaccinate), basic but very important epidemiological concepts when it comes to assessing the benefits and harms of any medical intervention, whether covid vaccines or Lipitor for your blood cholesterol (tip: the estimated NNV for covid vaccines is over 1,000, not promising to say the least). I have information to share if anybody is interested but I suspect there are epidemiologists in this forum much more apt than me to discuss this topic.
Claudia Chaufan, MD, PhD
Associate Professor, Health Policy & Global Health
Special Advisor to the Dean of Health in Curriculum Internationalization
School of Health Policy and Management
Graduate Program in Health
Global Health
Development Studies
Social and Political Thought
York University, Canada
https://shpm.info.yorku.ca/claudia-chaufan-new-faculty-profile/
"I would rather have questions that can't be answered than answers that can't be questioned.”
― Richard P. Feynman
From: Social Determinants of Health <[log in to unmask]> on behalf of Dennis Raphael <[log in to unmask]>
Sent: Friday, January 28, 2022 3:38 PM
To: [log in to unmask] <[log in to unmask]>
Subject: Vaccines don't work
https://www.nytimes.com/interactive/2021/us/covid-cases.html
And of course the very sick anti-vaxxers are killing others by clogging up hospitals and preventing needed care.
Get a free copy of Social Determinants of Health: The Canadian Facts, 2nd edition at http://thecanadianfacts.org
Join 1200+ health leaders on the SDOH Listserv at https://listserv.yorku.ca/archives/sdoh.html
Dennis Raphael, PhD
Professor of Health Policy and Management
York University
4700 Keele Street
Strong College, Room 334
Toronto, Ontario M3J 1P3
416-736-2100, ext. 22054
email: [log in to unmask]
Website: http://health.info.yorku.ca/health-profiles/index.php?mid=162284
Of interest:
The Politics of Health in the Canadian Welfare State
https://www.canadianscholars.ca/books/the-politics-of-health-in-the-canadian-welfare-state
Poverty in Canada, 3rd edition,
Forewords by Cathy Crowe, Rob Ranier and Jack Layton
https://www.canadianscholars.ca/books/poverty-in-canada-d3408482-0caa-489a-8a76-7faf7587d00a
Staying Alive: Critical Perspectives on Health, Illness, and Health Care, 3rd edition
Foreword by Gary Teeple
https://www.canadianscholars.ca/books/staying-alive
Social Determinants of Health: Canadian Perspectives, 3rd edition
Forewords by Michael Butler and Maude Barlow, Carolyn Bennett and Roy Romanow
http://tinyurl.com/hm5l4hn
Immigration, Public Policy, and Health: Newcomer Experiences in Developed Nations
http://www.cspi.org/books/immigration-public-policy-and-health
About Canada: Health and Illness, 2nd edition
https://fernwoodpublishing.ca/book/about-canada-health-and-illness
Tackling Health Inequalities: Lessons from International Experiences
Foreword by Alex Scott-Samuel
http://www.cspi.org/books/tackling_health_inequalities
Health Promotion and Quality of Life in Canada: Essential Readings
http://tinyurl.com/3C8zteu
See a presentation! The Political Economy of Health Inequalities.
http://www.youtube.com/watch?v=-NCTYqAub8g
Also, presentation at the University of Toronto on how Canada stacks up again other nations in providing citizens with economic and social security.
http://vimeo.com/33346501
See what Jack Layton had to say about my books!
http://www.cbc.ca/news/canada/story/2011/04/10/cv-election-ndp-layton-platform.html
at 27:20
To leave, manage or join list: https://listserv.yorku.ca/cgi-bin/wa?SUBED1=sdoh&A=1
To leave, manage or join list: https://listserv.yorku.ca/cgi-bin/wa?SUBED1=sdoh&A=1
To leave, manage or join list: https://listserv.yorku.ca/cgi-bin/wa?SUBED1=sdoh&A=1
To leave, manage or join list: https://listserv.yorku.ca/cgi-bin/wa?SUBED1=sdoh&A=1
To leave, manage or join list: https://listserv.yorku.ca/cgi-bin/wa?SUBED1=sdoh&A=1
|













{kind=link}
{kind=link}